


Part 5: How do we get insurance to cover learning differences?
Campaigning for Medicaid coverage of LDs

Part 3 outlined how families can put FSA dollars towards comprehensive evaluations and educational therapy but still be left with ~$5-10K in out-of-pocket costs annually. Part 4 discussed how LD-tech solutions theoretically increase access to treatment but are still costly. To truly shift the affordability paradigm, I believe Medicaid (and eventually private insurers) need to cover LD-related services.
Traditionally, we assume this type of policy decision is out of the businessperson’s control (Season 1 even said so!). However, if you better understand how political decision-making works, this assumption becomes an oversimplification. Herein, I’ll attempt to outline how the right campaign, run by a business, non-profit, or any organization with resources, could push Medicaid to cover comprehensive evaluations and ongoing educational therapy for LDs.
Why do LD-related services deserve coverage?
Affordability-aside, Medicaid should cover LDs because its clinically logical and because precedent exists.
First, think of the ‘LD-trickle down effect’ from Part 1. Properly treating LDs reduces the risk of mental health (i.e., anxiety, depression) and physical health issues (i.e., stemming from sleeping disturbances). As a result, though yet to technically be “proven”, I believe it’s logical to at least assume proper LD treatment could generate downstream cost savings.
Second, CMS requires Medicaid programs cover preventative and therapy services necessary to treat autism spectrum disorder (ASD), and Medicaid also covers ADHD medication[1]. ASD, ADHD, and LDs all meet the definition of “neurodevelopmental disorders”[2], and I’d argue LDs are more comparable to ASD and ADHD than most think.
Digging in further, as discussed in Part 1, LDs form when brain lobe(s) required to read, write, and/or do math are under-developed. Similarly, ADHD forms when brain lobes required for executive functions (e.g., self-control, emotional control) are under-developed. Last and in short, ASD originates from improperly developed folds/wrinkles in the brain that are required to “connect” information across different lobes and get them to working together[3].
Chart 1: Comparing ASD, ADHD, & LDs[4]

This comparison is not meant to oversimplify, but rather highlight the relationships across conditions. I acknowledge ASD, ADHD, and LDs are not equal, but at their core, they are quite comparable and that’s an important point to remember.
Why focus on Medicaid?
In addition to the precedent discussed above, Medicaid is a logical starting point for three reasons:
LD population size: When the public health emergency ends, ~33M+ children will still be covered by Medicaid or the Children’s Health Insurance Program (CHIP)[5]! CHIP provides coverage for children whose families earn too much to be Medicaid eligible. The Season 2 Teaser stated the prevalence of dyslexia, dysgraphia, and dyscalculia among children is 20%, 10%, and 5%, respectively. That means Medicaid coverage of LDs would create new treatment options for 6.6M, 3.3M, and 1.7M children (11.5M+ total!) that, today rely upon the Public School Path detailed in Part 2.
State-level control: States have some control over their Medicaid policies. Because of this, we can push for change at the state-level, which is significantly easier than at the federal-level where partisan gridlock often inhibits meaningful change.
De-stigmatization of Medicaid: Expanding Medicaid to cover families earning 138%+ of the Federal Poverty Limit (FPL) has been viewed favorably by most voters. A 2020 survey found that among those living in states yet to expand Medicaid, 61% wanted expansion[6]. That figure has likely has only increased as the pandemic shed greater light on Medicaid[7].
How do states add services to Medicaid?[8]
Medicaid is a federal-state partnership. It is jointly funded by states and the federal government and is administered by states in accordance with requirements established by the federal government.
Each state creates a ‘Medicaid State Plan’ (see New York’s) detailing eligibility requirements, services covered, etc., and this document is approved by the Department of Health & Human Services (HHS). Once approved, states can add new services covered by Medicaid in two ways:
State Plan Amendment (SPAs): Permanently adds new service for coverage. Does not need to be budget neutral.
Section 1115 Waiver: Temporarily allows for new services as part of a pilot/experiment. Must be budget neutral (i.e., cost with waiver can’t exceed costs without).
For this exercise, we’ll use an SPA to add LD services to the relevant Medicaid State Plan. Chart 2 below outlines how SPAs get approved:
Chart 2: State Plan Amendment (SPA) approval process[9]

Thus, for Medicaid to start covering comprehensive evaluations and ongoing educational therapy (via an SPA), three “political” tasks must be accomplished:
Task 1: Motivate the State Senate to pass a bill requiring the State Medicaid Agency submit the SPA
Task 2: Motivate the Governor to approve the SPA and urge CMS to approve the SPA
Task 3: Get CMS to approve the SPA
Precedent for Task 1 exists as Senate Bill 833 in California restored acupuncture as a Medicaid benefit in 2016. Further, to accomplish Task 1 and 2, both senators on the state’s health committee and the Governor must support the SPA.
I subscribe to the belief that *most* elected officials only act if they have an incentive to do so. Thus, any requested action must strengthen their re-election chances and/or inaction must decrease re-election chances. Altogether, to effectively motivate state senators and the Governor, a campaign must convince them the SPA will bolster their image, and advocates must be mobilized to the point inaction could impact their re-election chances.
Task 3, CMS approval, is less in a campaign’s control, but I’m convinced it won’t necessarily be the bottleneck. In Q1 2018, 84% of SPAs were approved by CMS in the first 90 days of review[11], and in 2021, New York submitted 33 SPAs for non-institutional services (i.e., services not delivered by hospital, long-term care facility, etc.) and was approved for 24 (or 72%) of them[12]. Not as bad as you thought, huh?!
The Campaign
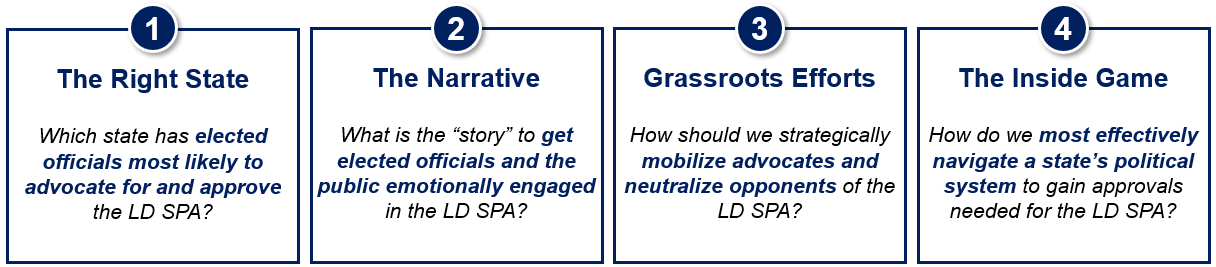
The right campaign can achieve Tasks 1 and 2 and get our LD SPA approved if it is anchored around the four tenets below.
Chart 3: Campaign tenets
For this exercise, let’s assume we are a startup, Orient Health (kudos to anyone who gets the multi-faceted pop culture reference)[13], providing virtual comprehensive evaluations and educational therapy. Orient believes serving the Medicaid population is critical to both its mission and growth, and our investors are willing to support a reasonably sized political campaign to gain Medicaid coverage of LDs.
The Right State
The first step is identifying the state where we think the greatest likelihood of SPA approval exists. To do so, we’ll apply five “filters” across all 50 states to find the right one.
I won’t bury the lead – we’re going to California! Chart 4 shows the output of the analysis, and text below describes each “filter” further.
Chart 4: State identification analysis

Filter 1 – Medicaid Expansion[14]: Has the state adopted the Affordable Care Act’s (ACA) expansion of Medicaid coverage for families earning up to 138% of FPL? An easy first filter as pushing for LD coverage in states still unwilling to expand Medicaid overall seems illogical.
Filter 2 – Continuous Coverage for Children[15],[16]: Has the state “opted-in”? If a child loses Medicaid eligibility (e.g., family income increases, they move, etc.), states can provide Medicaid coverage for an additional year. Thus, opting-in is a decent proxy for states’ willingness to add additional children-related benefits to Medicaid. Though it doesn’t impact the analysis, the 2022 Omnibus may make this continuing coverage mandatory.
Filter 3 – Party Rules: This campaign is about expanding social services, making it a partisan issue. The reality is, for any Republican to support our campaign, they must be willing to deviate from the GOP’s political agenda, and that is unlikely. Thus, we need a state where the Governor, Senate, and House are all Democrat.
Filter 4 – Economic Performance: Early in the ACA, states with weaker economies struggled to commit additional resources to Medicaid (despite financial incentives) [17]. The same logic holds here. We’ll assess state economic performance using the US News State Economy Rankings that considers new businesses, new patents, employment, growth (population and GDP). States 20th or below will be filtered out.
Filter 5 – Governor Connection: Making the final decision on which state to pursue is more of an art. Among the “Final Four” (California, Oregon, Washington, Colorado), we should select the state where the Governor has the strongest personal connection to LDs as this significantly increases our chances of getting the Governor to put some of their political weight behind us.
Chart 5: Governor connections to LDs[18],[19],[20],[21],[22]

Gavin Newsom struggled with dyslexia as a child, making California the winner. Colorado and Washington are also good candidates as both Governors have strong connections to LDs.
The Narrative
Orient heads to California! We now need a narrative to SELL elected officials and the public on why California NEEDS to cover LDs.
It’s critical to not overcomplicate the narrative. Overcomplicating, even if it leads to a stronger argument on paper, risks the public misunderstanding and the message getting diluted. The narrative must be simple enough to be broadly understood and powerful enough to get people emotionally charged. For example, a narrative built around the “LD-trickle down effect” from Part 1 seems logical; however, articulating the relationship between LDs and mental/physical health outcomes is too complex and not emotional enough.
One way to build a simple, but effective narrative is to anchor on three key, memorable points. In the case of California Medicaid covering LDs, that could be:
Better for children: More equitable access to LD treatment!
Better for teachers: Less disruptions in the classroom!
Better for Californians: A healthier and more productive population!
Below is a sample campaign poster bringing this to life, and the subsequent sections will dive into how different elements of the narrative get delivered via ‘Grassroots Efforts’ and ‘The Inside Game’.
Chart 6: Sample campaign poster

The Grassroots Efforts
To strategize grassroots efforts, we must 1) identify advocates and/or opponents (see Chart 7) and 2) based on their interests, determine ways to mobilize advocates and/or neutralize opponents.
Chart 7: The Medicaid & LDs “Playing Field”
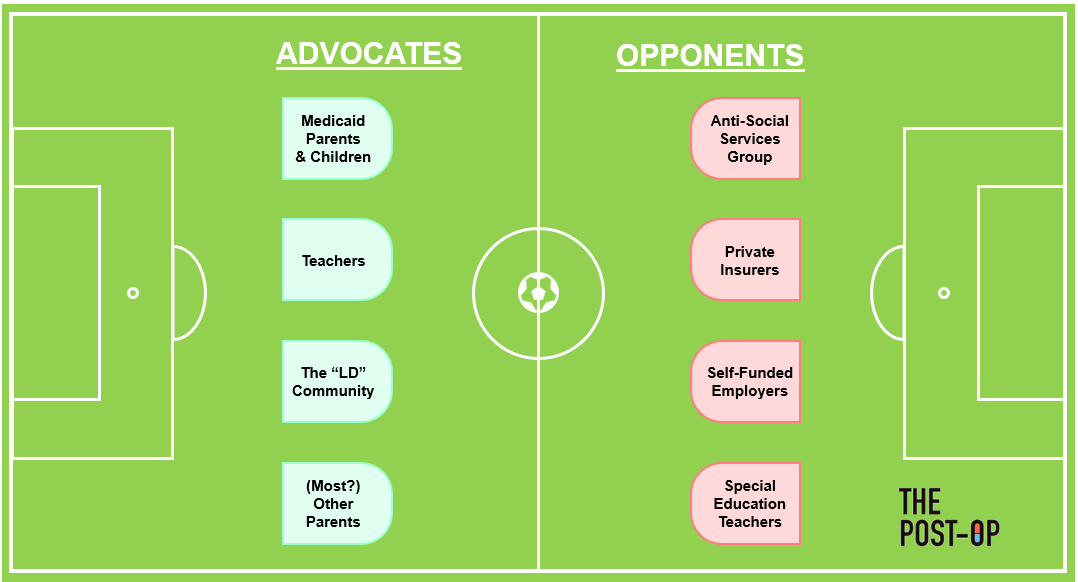
Advocates
Medicaid Parents & Children: They receive coverage for services (i.e., comprehensive evaluations, educational therapy) they otherwise couldn’t afford.
Teachers: Teacher-related benefits include more funding for general education (since less would be required for special education), fewer disruptions in the classroom (since LD students often require more attention), and fewer meetings overall. Teachers would also generally be thrilled for students to get better treatment than what schools provide.
The “LD Community”: Anyone with personal experience with LDs (i.e., themselves or loved ones) would presumably want to help others better address challenges they or loved ones likely faced.
(Most?) Other Parents: Motherly/fatherly instincts of current parents could trump political preferences and lead them to empathize with impacted families and children (and thus support the policy).
Mobilizing advocates is meant to push the California State Assembly, State Senate, and Governor Newsom to enact change (Task 1 & 2 from above). Again, if we believe most elected officials only act if it strengthens re-election chances or if not acting might cost them re-election, then the Assembly, Senate, and Governor view the most “important” advocates as the ones with control over their re-election chances! Thus, we must identify our strongest advocates that also have political and/or voting power and mobilize with them.
Mobilizing the Medicaid population would be the lowest-hanging fruit, but they lack the requisite voting power. Medicaid enrollee household income is typically less than $30,000, and Chart 8 illustrates how this group comprises less than 10% of the Democrat voting population.
Chart 8: Medicaid & the voting population[23],[24],[25]

The takeaway is we need to mobilize different advocates. Well, who has political and voting power? Unions! Are any of our advocates unionized? Yes! Teachers are. Here’s why activating the teacher’s union is critical[26]:
Scale: Teachers unions are massive and have money to spend on politics. For example, the California Teachers Association has 300K+ members and in 2022 alone, spent $5.5M+ fighting three major propositions.
Impact on Other Voters: Voters don’t see a distinction between the union and their local classroom teacher, meaning voters typically see the backing of a teacher’s union as a signal of support from their own community.
Nevertheless, on average, US elementary school teachers are 42 years old and 80%+ are female[27]. Thus, our grassroots efforts need to both be teacher-specific and tailored to this demographic group’s consumption patterns/tendencies. For example, of those in this age range, we know 74% use Facebook, 70% watch YouTube, 66% use streaming services, and 21% have cable[28],[29].
Opponents
Anti-Social Services Group: Those against taxes, and specifically taxes funding services like Medicaid, would not support increasing Medicaid’s cost burden by adding new services.
Private Insurers: Coverage by Medicaid could make private insurers feel obligated to add LD benefits, thereby increasing their overall cost of care.
Self-Funded Employers: Employers may feel obligated to add LD benefits otherwise they might appear indifferent to the needs of employees’ and their dependents/children.
Special Education Teachers: Demand for their services (delivered at public schools) would decline as many students could now receive treatment via privately practicing educational therapists.
The latter three groups are unlikely to present strong opposition. Private Insurers have some financial reasons to start providing LD benefits (discussed below), Self-Funded Employers probably want to avoid negative PR generated by opposing this policy, and Special Education Teachers still have the foundational skills needed to practice privately.
That leaves the Anti-Social Services Group as the primary opponents, and this group typically has financial resources and influence necessary to steer elected officials. Though less of an issue in California, the Anti-Social Services Group is probably too strong to be neutralized. Thus, it would be more efficient/effective if our grassroots tactics focused on strengthening the voice of our advocates (i.e., teachers) rather than battling opponents.
Grassroots Tactics
Based on the “playing field” dynamics, our general strategy for grassroots tactics will be:
Generate “conviction-strengthening” content
Deliver content through channels and at times (i.e., the summer) best suited to reach the target advocates – teachers
Strengthen conviction of the teachers and teacher’s unions (the California Teachers Association in this scenario)
Here are some examples tactics for generating “conviction-strengthening” content:
Famous Spokesperson: Have a famous person relevant to the teachers’ demographic in ads supporting the issue. Keanu Reeves and Jennifer Aniston both struggled with LDs[30],[31]!
General Campaign: Inform teachers of the proposed policy and accompanying narrative
Teacher Testimonials: Get current teachers speaking out about how the current system takes money from and disrupts general education
“Success” Stories: Highlight students whose lives were turned around once they started seeing an educational therapist
“Failure” Stories: Highlight examples of harm caused by students who lacked access to LD-treatment – sadly some school shootings have been linked to inadequate LD treatment (e.g., Uvalde). I don’t subscribe to this tactic, but felt it was worth mentioning
Call for Letters to Politicians: Push teachers to write letters to their elected officials asking for their support of this policy
Chart 9 illustrates how, based on the tendencies of teachers, we can most effectively deliver this content and mobilize them as advocates.
Chart 9: Advocate mobilization tactics by channel
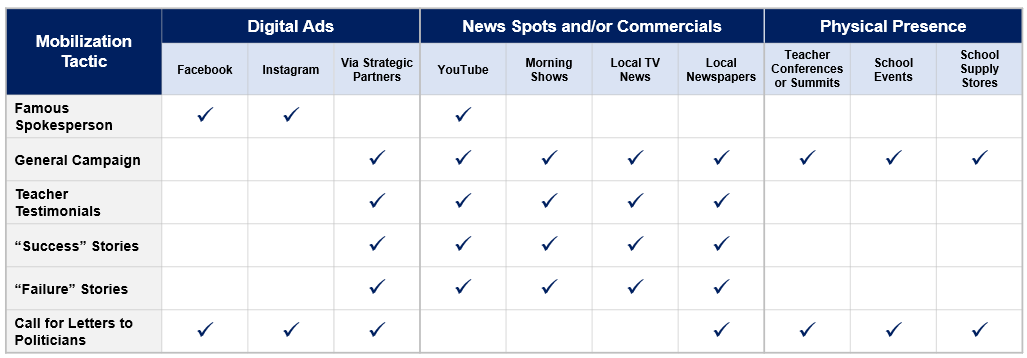
Two unique channels necessitating further elaboration:
Strategic Partners implies collaborating with a high-traffic platform for teachers (e.g., Google Classroom, Canvas, Teachers Pay Teachers, SeeSaw) and working together to deliver tactics digitally via their email list, website, teacher portals, etc.
Physical Presence involves delivering a “mobilization tactic” by putting up posters, handing out fliers, setting up a “booth”, etc. School Events include sporting events, school performances, etc. School Supply Stores include stores like Lakeshore Learning Materials, Walmart, Staples, etc.
Nevertheless, the ‘Grassroots Efforts’ need to generate enough support and noise that Medicaid covering LDs becomes an issue the California State Senate is willing to consider. At that point, we can begin to play ‘The Inside Game’.
The Inside Game
To reiterate, politically, we need the California Senate Health Committee to pass a bill requiring the California State Medicaid agency (i.e., California Department of Health Care Services) submit an SPA to Gavin Newsom and we need Newsom to support and advocate for the SPA. The process of passing a bill is nuanced and varies state-to-state. In general, it requires starting with a lower house (e.g., California State Assembly) before moving to an upper house (e.g., California State Senate) and eventually to the Governor[32]. We’ll follow that approach, but for the purposes of this exercise, we won’t be diving any further into legislative technicalities.
Step 0 – Scheduling the Meeting: To get a meeting in the first place, Assembly Members or Senators need to believe this bill is worth their time. For them something to be worth their time, money and/or votes need to be at-stake. If our grassroots efforts are successful, Assembly Members and/or Senators will realize that donations and votes from the California Teachers Association would be at-risk if they don’t support the bill and thus should be willing to take a meeting.
Step 1 – Gaining Health Committee Support: In addition to articulating how money and/or votes are at-stake, in these meetings, we must sell them on our campaign by articulating the narrative and illustrating the scope of LDs at schools in their district. It requires research and creativity, but powerful data points to highlight might include:
“Invisible Children”: Number of students in IEPs compared to what we’d expect based on national prevalence
Capacity Constraints: Special educators and/or psychologists per student relative to benchmarks
Real Stories: Testimonials from parents and teachers in their district that navigated IEP processes
Step 2 – Acquiring an Inside Man or Woman: To maximize credibility before meeting the Governor, our campaign needs strong advocate(s) on the inside with political clout in the state. This could be the Senate President, the Majority Whip, the Chair of the CA Senate Health Committee, or even Senate Health Committee members if needed. In general, we’d want to scan the CA State Senate to find individuals that wield significant power, have personal ties to LDs, and are Medicaid expansion advocates. Once identified, we’d repeat Steps 0 & 1 to get them bought in on the bill.
Step 3 – Gaining Governor Support: As mentioned, Gavin Newsom has dyslexia, increasing the likelihood the narrative resonates. If we have legitimate support of the bill from the California Teachers Association, the State Assembly, and the State Senate, then we probably just need the Governor’s “rubber stamp” (i.e., not vetoing the bill). However, in instances when we need to “sway” the Governor, messaging needs to be quite strategic, so the checklist below provides everything you’d want to consider/include in that pitch:
Chart 10: The Governor meeting checklist

And there you have it! This strategic combination of ‘Grassroots Efforts’ and ‘The Inside Game’ is the path Orient Heal would likely need to take get the Governor to approve the bill requiring the State Medicaid Agency draft an SPA requiring Medicaid cover comprehensive evaluations and ongoing educational therapy for LDs. I’m tired.
Rapid-fire
I want to close with three rapid-fire rounds on the following as it relates to Medicaid & LDs: 1) future challenges, 2) private insurers, and 3) private practice implications.
Future challenges
Thoughts on the biggest challenges that would remain even after a successful campaign:
Medicaid Population: Despite “coverage”, Medicaid still needs to design networks, define cost sharing, and set prior authorization requirements, which all limit access.
Non-Medicaid Population: There’s still a “donut hole” where families earn too much to be eligible for Medicaid, but too little to afford paying out-of-pocket for private practice LD services.
Scalability: Financing a campaign like this is costly and difficult to scale as no two states Medicaid program and politics are the same.
Private insurance coverage
Thoughts on the why private insurers may be receptive to covering LDs:
Growth!: Covering LDs increases cost of care, but gives reason to increase premiums to off-set said cost and thus grow revenue and total gross margin ($). Theoretically, LDs increase total cost of care across a family by $46 per person per month (see math here). Chart 11 reflects how that $46 could be pushed through via premiums while keeping gross margin (%) steady.
Chart 11: LD financial impact on private insurers

Employer Offering: Children with LDs are often dependents on their parent’s employer-sponsored insurance. Thus, employers might be willing to add LD-related benefits to better “care for” their employees.
Private practice implications
Non-exhaustive thoughts on how, downstream, Medicaid coverage for LDs would impact private practices:
Prices: No longer living in cash-pay world, prices for assessments and treatment would increase to offset greater administrative expenses (i.e., from billing Medicaid).
Administrative Tasks: Neuropsychologists and educational therapists will need to learn how to properly document interactions and submit bills to Medicaid for reimbursement.
Protocols: If the state is paying for these services, there would need to be more clearly defined certifications and quality/outcomes-related metrics that currently don’t exist.
Parting shot
First off, this was a 90-minute finale for a season with 30-minute episodes, so if you’ve made it this fair, I appreciate it!
Next, if you are thinking to yourself, hmm the level of effort and investment required to enact a new Medicaid policy is insane, you’re right! It is insane, but I wanted to outline how an opportunity does exist to strategically leverage our political system to enact healthcare change we wish to see.
Anyway, that’s a wrap on Season 2! As mentioned, my primary goal was to spread awareness about LDs to the healthcare community, so I hope you are now a healthcare professional much more informed on dyslexia, dysgraphia, and dyscalculia than you were six weeks ago.
Last, I have been working on Season 1 & 2 of The Post-Op for the last 7+ months, so I will be going on hiatus for a bit. I graduate from Columbia Business School in May and start working full-time again this summer, so we’ll see what ideas pop into my head between now and then.
**
Links to: Sources | Graphics (PPT) | Analyses (Excel)
Personal Links: Twitter | LinkedIn | Modeling Inquiries
For more on Medicaid technicalities, read HealthTechNerd’s overview here. For more on strategically navigating regulation, read The Fixer by Bradley Tusk, famed political consultant and professor of mine.