


Part 4: A look at the Learning Difference-Tech ecosystem
Who’s building to transform the learning difference status quo?

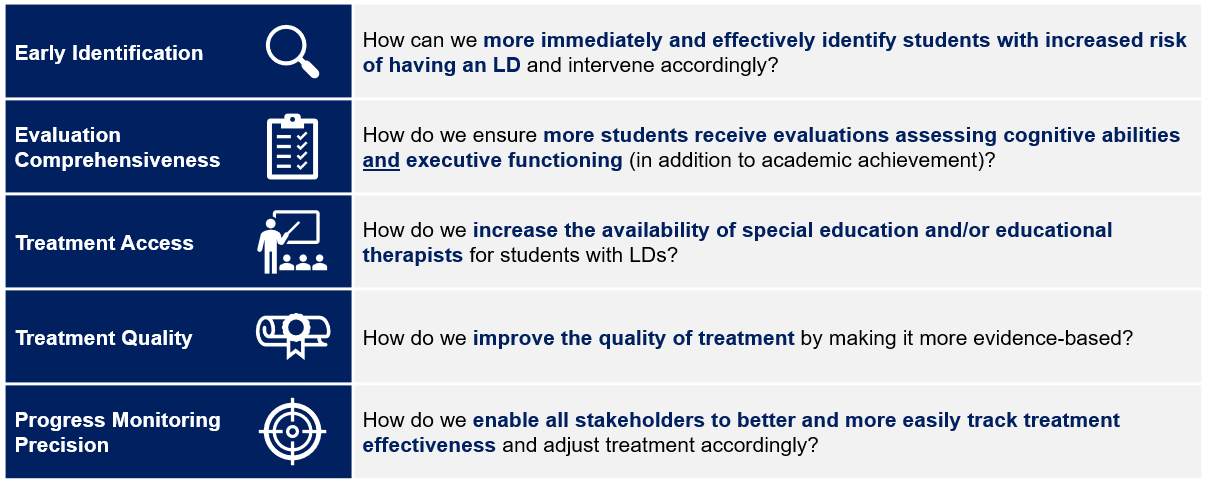
To me, transforming the LD status quo would mean all students have access to effective treatment as early as possible, and I believe there are five keys necessary to facilitating said transformation.
Chart 1: The Five Keys to Learning Difference Transformation
Part 2 and Part 3 discussed public schools and private practices in the context of the five keys to transformation, but there are also various software and technology-enabled services businesses building solutions to transform the LD status quo as well.
Chart 2: The LD-Tech Ecosystem[1]

Season 2 has emphasized how LDs sit at the intersection of healthcare and education, and the LD-Tech ecosystem is no different. To ensure you walk away understanding the space, we’ll highlight the following for each segment:
Keys to Transformation Addressed (icons in top right)
Products and/or Services
Business Model
One Takeaway (for building, investing, etc.)
For Students & Families (B2C):

Products and/or Services[2],[3],[4]: Screening tools have students complete a digital assessment to predict the likelihood an LD exists or to identify cognitive strengths/weaknesses. dystech’s dyslexia prediction is based on students’ performance on a 5-minute reading test and voice recordings! EarlyBird’s 30-minute game tests 12 areas known to predict reading ability (e.g., letter sound, word matching). MindPrint focuses more on assessing cognitive skills.
Graphic 1: Screening tool screenshots[5],[6]

Business Model[7],[8],[9]: dystech, EarlyBird, and Mindprint all charge per-screening – $13, $299, and $199 each, respectively. dystech is Australia-based, likely explaining the discrepancy. Each also sell their tool to districts/schools whose educators administer the screening. Some Curriculum Providers (discussed later) offer similar tools, too.
One Takeaway: Intriguing if you’re looking to start an LD business or side-hustle. The segment presents a clear (albeit tricky) software use case with a large TAM, the space is still nascent (i.e., no tools for dysgraphia or dyscalculia), and there is a logical exit via acquisition by Evaluation Platforms or Educational Therapy Platforms.

Products and/or Services: These platforms bring the ‘Private Practice Evaluation’ from Part 3 online. Through multiple 1-on-1 sessions conducted virtually (lasting 5+ hours total), each performs a comprehensive evaluation on students, testing cognitive abilities and executive functioning before providing diagnosis/documentation required to inform IEP/504 eligibility.
Business Model[10]: Platforms charge per-evaluation with the evaluation and pricing varying as outlined below.
Chart 3: Comparison of Evaluation Platforms[11],[12],[13]
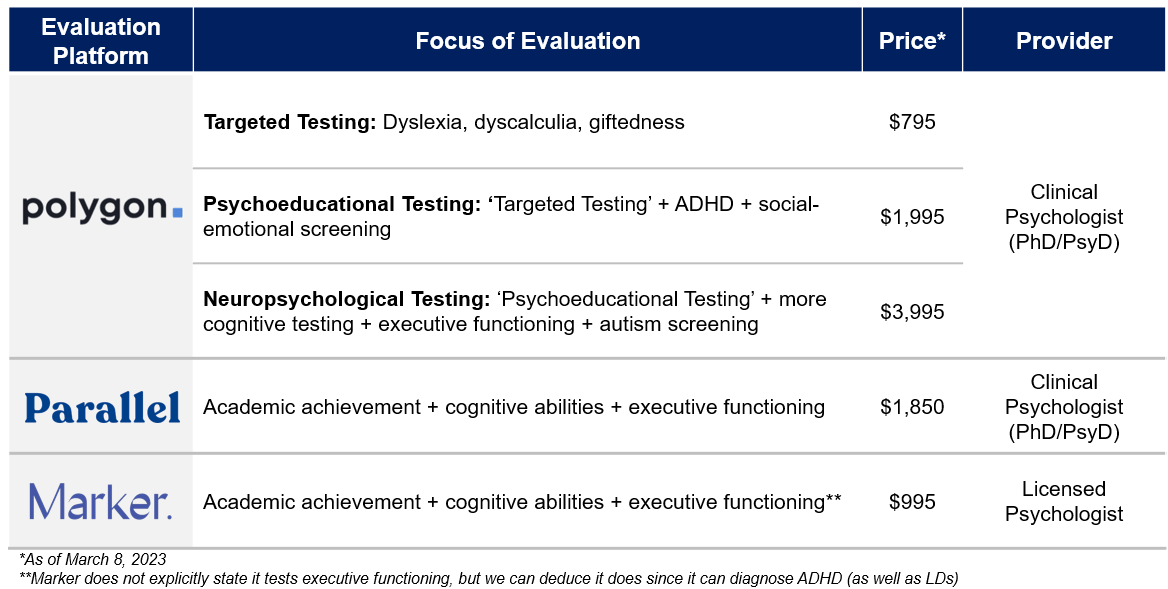
One Takeaway: Strong product-market fit, theoretically. Private practice neuropsychologist evaluations are expensive (i.e., $8K+ in some areas discussed in Part 3) and often inaccessible (i.e., in-person only, working hours only). These platforms solve the cost and access problem with competitive pricing (though still expensive), virtual experience, and flexible hours.

Products and/or Services[14],[15],[16]: Educational Therapy Platforms bring the practice of educational therapy online with greater scale. Following evaluation, students are matched with an educational therapist/learning specialist[17] typically trained to deliver evidence-based, multisensory programs like Orton-Gillingham. Most deliver treatment via 1-on-1 virtual sessions. Learnfully also offers group-based learning and Brain Balance, with 80+ centers nationwide, offers in-person treatment options.
Business Model[18]: Platforms provide a free initial consultation and most commonly sell session packages. For example, Parallel charges $150/month for 2 sessions and $292/month for 4 sessions. These platforms also serve more than LDs, offering treatment options for behavioral health (e.g., anxiety), executive function (i.e., ADHD), and speech.
One Takeaway[19]: Potential to be disruptive to traditional private practices. Platforms benefit from modern technological architecture (and cleaner data collection), making it easier to deliver personalized treatment and proactively monitor progress. Their scale enables competitive pricing (i.e., in the first quartile from Part 3 at ~$75/session), but although counterintuitive, lower pricing could imply lower quality, making parents less likely buyers. Also, maintaining quality and intimacy with families amidst investor growth expectations will be critical to longer-term success.

Products and/or Services[20],[21],[22]: Elea supports families via its ‘Caregiver Portal’ for special needs documentation management, via its care concierges for navigating special needs processes, and via its ‘Village Community’ for connecting with other caregivers and special needs experts. For students, various “assistive technologies” help better manage LDs. Speechify can turn text into speech; Co:Writer comprehends context to auto-complete words and identify grammar issues; Microsoft Math Solver solves math problems with just a picture of the problem!
Business Model(s): Elea charges families $10 per-month for its ‘Caregiver Portal’. Assistive technology revenue models vary by product, ranging from one-time hardware purchases (e.g., digital highlighters) to monthly subscription fees to even free.
One Takeaway: (Assistive Technology) Proceed with caution. Assistive technologies make LDs more manageable, but as the technology becomes smarter, more accessible, and more capable of completing assignments for students (e.g., Chat GPT-3), it could make identifying LDs even more difficult.
For Schools (B2B or B2B2C)

Products and/or Services[23],[24],[25]: Curriculum Providers sell programs (i.e., digital ‘assignments’) to schools to give students with LDs. Assignments are purpose-built to strengthen components proven to improve reading ability (e.g., sound/symbol association), are supposedly more “fun”, and are completed via laptop/tablet. The value proposition is largely that, because the assignments are digital, they can adapt/be personalized based on individual students’ performance and they can automate data collection, allowing teachers to track progress more easily. Amplify also offers a screening tool (like Graphic 1) as part of its curriculum.
Graphic 2: Curriculum screenshot[26]

Business Model: Curriculum Providers today only offer dyslexia-focused curriculum, which they sell to districts/schools whose special educators deliver it to students. Pricing is opaque but charging per-student seems most likely. For example, TeachTown, an autism-focused curriculum provider, charges $299 per-student annually.
One Takeaway: Distribution is key. Even with transformational curriculum and/or reporting capabilities, ‘Curriculum Providers’ must convince districts/public schools to buy it. Districts/schools must train educators to administer it and potentially convince them of its value, too, and educators must ensure students use it properly and are not distracted by it. The LD-Tech B2B2C model!

Products and/or Services[27],[28],[29]: Service Providers sell virtual evaluation and/or special education services directly to schools lacking either capacity or technological capabilities required to deliver it themselves. Services are also oftentimes offered alongside a case management and reporting platform. Chart 4 breaks down the players.
Chart 4: Service Provider breakdown

Business Model: Like its direct-to-family offering, Polygon charges schools the same rates and services as in Chart 3. Parallel and TeleTeachers don’t publicize revenue models, but presumably charge per-session and/or monthly subscriptions for a certain number of sessions.
One Takeaway: Hazier product-market fit. To elect to outsource to a Service Provider, districts would likely either need to quickly:
Offer special education services virtually OR
Increase special educator capacity and choose to do so by contracting a third-party rather than re-allocating existing capacity across schools
#1 seems less likely post-COVID while #2 seems expensive and inefficient.

Products and/or Services[30],[31]: Part 2 outlined tasks necessary to create IEPs (e.g., evaluation, meetings, etc.) and details required to be included (e.g., performance, goals, accommodations, etc.). ‘IEP Management Platforms’ are the digital system of record for managing/completing those tasks and storing that data. Platforms can also flag errors in the IEP for information gaps or compliance issues and/or facilitate Medicaid billing when eligible services are performed.
Business Model: Platforms operate as SaaS businesses as they are typically web-based and charge districts/schools based on the number of students tracked. Vendors highlighted above did not publish pricing.
One Takeaway: The EHR of special education.

Products and/or Services[32],[33]: Tracking IEPs can be tedious (potentially paper-based) and challenging to maintain in real-time. LiftEd strives to be a user-friendly platform educators can use to enter student data and monitor progress (e.g., add reading fluency assessment scores then see score’s 3-month trend). mytaptrack seeks to facilitate real-time data collection as educators click a button on a handheld device where number of clicks corresponds to certain behaviors (e.g., two clicks = child distracted).
Business Model[34],[35]: Both use different variations of subscriptions. LiftEd charges $299 per-teacher per year for the platform plus training/implementation while mytaptrack charges per-device, bundled with a 12-month license accessible for all teachers.
One Takeaway: (LiftEd) Interesting exit potential despite unclear moat. LiftEd seemingly has a user experience competitive advantage that could (and should) be replicated by IEP Management Platforms. However, it may be easier for IEP Management Platforms to buy rather than build a new data collection layer, making LiftEd a logical acquisition target.
Parting shot
If you believe students stand to benefit the more LDs are managed outside of schools, then families and students must be adequately empowered to address the issues they face around early identification, therapist availability, and treatment quality. The B2C segment is striving to solve these issues in a family-friendly manner, and that excites me. Sadly though, and I’m going to sound like a broken record here, it’s still too expensive for most to afford out-of-pocket.
**
Links to: Sources | Graphics (PPT)
If you want to chat further about LDs or anything healthcare-related, follow me on Twitter @z_miller4 or connect with me on LinkedIn!
If you are an early-stage startup and potentially interested in my support for any unit economics or financial modeling-related activities, please fill out the form here.
Great read!